Methylprednisolone sodium succinate.
Each vial contains: Methylprednisolone (as methylprednisolone sodium succinate) 1g.
The reconstituted solution is clear and colourless.
Pharmacology: Mechanism of Action: Glucocorticoids diffuse across cell membranes and complex with specific cytoplasmic receptors. These complexes then enter the cell nucleus, bind to DNA (chromatin), and stimulate transcription of mRNA and subsequent protein synthesis of various enzymes thought to be ultimately responsible for the numerous effects of glucocorticoids after systemic use. Glucocorticoids not only have an important influence on inflammatory and immune processes, but also affect the carbohydrate, protein and fat metabolism. They also act on the cardiovascular system, the skeletal muscles and the central nervous system.
Effect on the inflammatory and immune process: The anti-inflammatory, immunosuppressive and anti-allergic properties of glucocorticoids are responsible for most of the therapeutic applications. These properties lead to the following results: Reduction of the immunoactive cells near the inflammation focus; Reduced vasodilation; Stabilization of the lysosomal membranes; Inhibition of phagocytosis; Reduced production of prostaglandins and related substances. A dose of 4mg methylprednisolone has the same glucocorticosteroid (anti-inflammatory) effect as 20mg hydrocortisone. Methylprednisolone has only a minimal mineralocorticoid effect (200mg methylprednisolone are equivalent to 1mg desoxycorticosterone).
Effect on carbohydrate and protein metabolism: Glucocorticoids have a protein catabolic action. The liberated amino acids are converted into glucose and glycogen in the liver by means of the gluconeogenesis process. Glucose absorption in peripheral tissues decreases, which can lead to hyperglycemia and glucosuremia, especially in patients who are prone to diabetes.
Effect on fat metabolism: Glucocorticoids have a lipolytic action. This lipolytic activity mainly affects the limbs. They also have a lipogenetic effect which is most evident to chest, neck and head. All this leads to a redistribution of the fat deposits. Maximum pharmacologic activity of corticosteroids lags behind peak blood levels, suggesting that most effects of the drugs result from modification of enzyme activity rather than from direct actions by the drugs.
Pharmacokinetics: In vivo, cholinesterases rapidly hydrolyse methylprednisolone sodium succinate to free methylprednisolone. In man, methylprednisolone forms a weak dissociable bond with albumin and transcortin. Approximately 40 to 90% of the drug is bound. Intravenous infusions with 30mg/kg, administered over 20 minutes or 1g administered over 30 to 60 minutes lead after approximately 15 minutes to peak methylprednisolone plasma levels of nearly 20lg/ml. About 25 minutes after an intravenous bolus injection of 40mg peak methylprednisolone plasma levels of 34lg/100ml after some 120 minutes. Intramuscular injections give lower peak values than intravenous injections. With I.M. injections plasma values persist for a longer period, with the result that both administration patterns lead to equivalent quantities of methylprednisolone. The clinical importance of these small differences is probably minimal when we consider the mechanism of action of glucocorticoids. A clinical response is usually observed 4 to 6 hours after administration. In the treatment of asthma, the first beneficial results can already be perceived after 1 or 2 hours. The plasma half-life of methylprednisolone sodium succinate is 2.3 to 4 hours and appears to bear no relation to the administration pattern. Methylprednisolone is a glucocorticoid with a medium-term activity. It has a biological half-life of 12 to 36 hours. The intracellular activity of glucocorticoids results in a clear difference between plasma half-life and pharmacological half-life. Pharmacological activity persists after measurable plasma levels have disappeared. The duration of anti-inflammatory activity of glucocorticoids approximately equals the duration of hypothalamic-pituitary-adrenal (HPA) axis suppression. Metabolism of methylprednisolone occurs via hepatic routes qualitatively similar to that of cortisol. The major metabolites are 20 beta-hydroxymethylprednisolone and 20 beta-hydroxy-6 alpha-methylprednisone. The metabolites are mainly excreted in the urine as glucuronides, sulfates and unconjugated compounds. Following I.V. administration of 14C labeled methylprednisolone, 75% of the total radioactivity was recovered in the urine in 96 hours, 9% was recovered in human feces after 5 days and 20% in the bile.
Glucocorticoids should only be considered as a purely symptomatic treatment, unless in case of some endocrine disorders, where they are used as substitution treatment.
Anti-Inflammatory Treatment: Rheumatic Disorders: As adjunctive therapy for short-term administration (to tide the patient over an acute episode or exacerbation) in: Post-traumatic osteoarthritis; Synovitis or osteoarthritis; Rheumatoid arthritis including juvenile rheumatoid arthritis (selected cases may require low-dose maintenance therapy); Acute and subacute bursitis; Epicondylitis; Acute non-specific tenosynovitis; Acute gouty arthritis; Psoriatic arthritis; Ankylosing spondylitis.
Collagen Diseases: During an exacerbation or as maintenance therapy in selected cases of: Systemic lupus erythematosus; Acute rheumatic carditis; Systemic dermatomyositis (polymyositis); Polyarteritis nodosa; Good pasture's syndrome.
Dermatologic Diseases: Pemphigus; Severe erythema multiforme (Stevens-Johnson syndrome); Exfoliative dermatitis; Bullous dermatitis herpetiformis; Severe seborrheic dermatitis; Severe psoriasis; Mycosis fungoides; Urticaria.
Allergic States: Control of severe or incapacitating allergic conditions intractable to adequate trials of conventional treatment in: Bronchial asthma; Contact dermatitis; Atopic dermatitis; Serum sickness; Seasonal or perennial allergic rhinitis; Drug hypersensitivity reactions; Urticarial transfusion reactions; Acute non-infectious laryngeal oedema (epinephrine is the drug of first choice).
Ophthalmic Diseases: Severe acute and chronic allergic and inflammatory processes involving the eye, such as: Herpes zoster ophthalmicus; Iritis, iridocyclitis; Chorioretinitis; Diffuse posterior uveitis and choroiditis; Optic neuritis; Sympathetic ophthalmia.
Gastrointestinal Diseases: To tide the patient over a critical period of the disease in: Ulcerative colitis (systemic therapy); Crohn's disease (systemic therapy).
Respiratory Diseases: Symptomatic pulmonary sarcoidosis; Berylliosis; Fulminating or disseminated pulmonary tuberculosis when used concurrently with appropriate anti-tuberculous chemotherapy; Loeffler's Syndrome not manageable by other means; Aspiration pneumonitis.
Edematous states: To induce diuresis or remission of proteinuria in the nephritic syndrome, without uremia, of the idiopathic type or that due to lupus erythematosus.
Immunosuppressive Treatment: Organ transplantation.
Treatment of Hematological and Oncological Disorders: Hematologic Disorders: Acquired (autoimmune) haemolytic anemia; Idiopathic thrombocytopaenia purpura in adults (IV only; IM administration is contraindicated); Secondary thrombocytopenia in adults; Erythroblastopenia (RBC anemia); Congenital (erythroid) hypoplastic anemia.
Oncological Diseases: For palliative management of: Leukemias and lymphomas; Acute leukemia of childhood.
Treatment of Shock States: Shock secondary to adrenocortical insufficiency or shock unresponsive to conventional therapy when adrenal cortical insufficiency may be present. (Hydrocortisone is generally the drug of choice. When mineralocorticoid activity is undesirable, methylprednisolone may be preferred.) Hemorrhagic, traumatic and surgical shock unresponsive to standard therapy.
Although there are no well-controlled (double-blind placebo) clinical trials, data from experimental animal models indicate that methylprednisolone sodium succinate may be useful in shock states in which standard therapy e.g. fluid replacement has not been effective.
Others: Nervous System: Cerebral oedema from tumour - primary of metastatic and/or associated with surgical or radiation therapy or head trauma; Acute exacerbations of multiple sclerosis; Acute spinal cord injury - the treatment should begin within eight hours of injury; Tuberculous meningitis with subarachnoid block or impending block when used concurrently with appropriate anti-tuberculosis chemotherapy; Trichinosis with neurologic or myocardial involvement; Prevention of nausea and vomiting associated with cancer chemotherapy.
Endocrine Disorders: Primary or secondary adrenocortical insufficiency; Acute adrenocortical insufficiency; For these indications, the drugs of choice are hydrocortisone or cortisone. Synthetic analogues can be used in certain circumstances if they are combined with mineralocorticoids; Preoperatively and in the event of serious, trauma or illness, in patients with known adrenal insufficiency or when adrenocortical reserve is doubtful; Congenital adrenal hyperplasia; Nonsuppurative thyroiditis; Hypercalcaemia associated with cancer.
Methylprednisolone sodium succinate may be administered by intravenous (IV) injection or infusion, or by intramuscular (IM) injection. The preferred method for initial emergency use is IV injection. Dosage may be reduced for infants and children but should be selected based on the severity of the condition and the response of the patient rather than on the age or weight of the patient. The pediatric dosage should not be less than 0.5mg/kg every 24 hours.
Adjunctive therapy in life threatening conditions: Administer 30mg/kg IV over a period of at least 30 minutes. Dose may be repeated every 4 to 6 hours for up to 48 hours.
Rheumatic disorders unresponsive to standard therapy (or during exacerbation episodes): 1g/day for 1 to 4 days, or 1g/month for 6 months. Administer either regimen as IV pulse dosing over at least 30 minutes. The regimen may be repeated if improvement has not occurred within a week after therapy, or as the patient's condition dictates.
Systemic lupus erythematosus unresponsive to standard therapy (or during exacerbation episodes): Administer 1g/day for 3 days as IV pulse dosing over at least 30 minutes. The regimen may be repeated if improvement has not occurred within a week after therapy, or as the patient's condition dictates.
Multiple sclerosis unresponsive to standard therapy (or during exacerbation episodes): Administer 1g/day for 3 or 5 days as IV pulse dosing over at least 30 minutes. The regimen may be repeated if improvement has not occurred within a week after therapy, or as the patient's condition dictates.
Prevention of nausea and vomiting associated with cancer chemotherapy: For mild to moderately emetogenic chemotherapy: Administer 250mg IV over at least 5 minutes 1 hour before start of chemotherapy. Repeat dose of methylprednisolone at the initiation of chemotherapy and at the time of discharge. A chlorinated phenothiazine may also be used with the first dose of methylprednisolone for increased effect.
For severely emetogenic chemotherapy: Administer 250mg IV over at least 5 minutes with appropriate doses of metoclopramide or a butyrophenone 1 hour before start of chemotherapy. Repeat dose of methylprednisolone at the initiation of chemotherapy and at the time of discharge.
Acute spinal cord injury - Treatment should begin within 8 hours of injury: For patients initiated on treatment within 3 hours of injury: Administer 30mg/kg as an IV bolus over a 15-minute period, followed by a 45 minute pause, and then a continuous IV infusion of 5.4mg/kg/h for 23 hours.
For patients initiated on treatment within 3 to 8 hours of injury: Administer 30mg/kg as an IV bolus over a 15-minute period, followed by a 45-minute pause, and then a continuous IV infusion of 5.4mg/kg/h for 47 hours. There should be a separate intravenous site for the infusion pump.
As adjunctive therapy in other indications: Initial dose will vary from 10 to 500mg IV, depending on the clinical condition. Larger doses may be required for short-term management of severe, acute conditions. Initial doses up to 250mg should be administered IV over a period of at least 5 minutes, while larger doses should be administered over at least 30 minutes. Subsequent doses may be administered IV or IM at intervals dictated by the patient's response and clinical condition. To avoid compatibility and stability problems, it is recommended that methylprednisolone sodium succinate be administered separately from other drugs whenever possible, as either IV push, through an IV medication chamber, or as an IV "piggy-back" solution.
Reconstitution: Under aseptic conditions, add the bacteriostatic water for injection to the vial with sterile powder. If desired, the medication may be administered in dilute solutions by admixing the reconstituted product with dextrose 5% in water, normal saline, dextrose 5% in 0.45% sodium chloride. The resulting solutions are physically and chemically stable for 48 hours.
There is no clinical syndrome of acute overdosage with corticosteroids. Reports of acute toxicity and/or death following overdosage of corticosteroids are rare. In the event of overdosage, no specific antidote is available; treatment is supportive and symptomatic. Methylprednisolone is dialysable. Following chronic overdosage the possibility of adrenal suppression should be guarded against by gradual diminution of dose levels over a period of time. In such event the patient may require to be supported during any further stressful episode.
Methylprednisolone is contraindicated: in patients who have systemic fungal infections unless specific anti-infective therapy is employed and in cerebral oedema in malaria; in patients with known hypersensitivity to methylprednisolone or any component of the formulation; for use by the intrathecal route of administration. Administration of live or live, attenuated vaccines is contraindicated in patients receiving immunosuppressive doses of corticosteroids.
Immunosuppressant Effects/Increased Susceptibility to Infections: Corticosteroids may increase susceptibility to infection, may mask some signs of infection, and new infections may appear during their use. Suppression of the inflammatory response and immune function increases the susceptibility to fungal, viral and bacterial infections and their severity. The clinical presentation may often be atypical and may reach an advanced stage before being recognised. Persons who are on drugs which suppress the immune system are more susceptible to infections than healthy individuals. Chicken pox and measles, for example, can have a more serious or even fatal course in non-immune children or adults on corticosteroids. Chickenpox is of serious concern since this normally minor illness may be fatal in immunosuppressed patients. Patients (or parents of children) without a definite history of chickenpox should be advised to avoid close personal contact with chickenpox or herpes zoster and if exposed they should seek urgent medical attention. Passive immunization with varicella/zoster immunoglobin (VZIG) is needed by exposed non-immune patients who are receiving systemic corticosteroids or who have used them within the previous 3 months; this should be given within 10 days of exposure to chickenpox. If a diagnosis of chickenpox is confirmed, the illness warrants specialist care and urgent treatment. Corticosteroids should not be stopped and the dose may need to be increased. Exposure to measles should be avoided. Medical advice should be sought immediately if exposure occurs. Prophylaxis with normal intramuscular immunoglobulin may be needed. Similarly, corticosteroids should be used with great care in patients with known or suspected parasitic infections such as Strongyloides (threadworm) infestation, which may lead to Strongyloides hyperinfection and dissemination with widespread larval migration, often accompanied by severe enterocolitis and potentially fatal gram-negative septicemia. Although methylprednisolone is not approved in the UK for use in any shock indication, the following warning statement should be adhered to. Data from a clinical study conducted to establish the efficacy of methylprednisolone in septic shock, suggest that a higher mortality occurred in subsets of patients who entered the study with elevated serum creatinine levels or who developed a secondary infection after therapy began. Therefore this product should not be used in the treatment of septic syndrome or septic shock. The role of corticosteroids in septic shock has been controversial, with early studies reporting both beneficial and detrimental effects. More recently, supplemental corticosteroids have been suggested to be beneficial in patients with established septic shock who exhibit adrenal insufficiency. However, their routine use in septic shock is not recommended. A systematic review of short-course, high-dose corticosteroids did not support their use. However, meta-analyses, and a review suggest that longer courses (5-11 days) of low-dose corticosteroids might reduce mortality. Live vaccines should not be given to individuals with impaired immune responsiveness. The antibody response to other vaccines may be diminished. The use of corticosteroids in active tuberculosis should be restricted to those cases of fulminating or disseminated tuberculosis in which the corticosteroid is used for the management of the disease in conjunction with an appropriate anti-tuberculous regimen. If corticosteroids are indicated in patients with latent tuberculosis or tuberculin reactivity, close observation is necessary as reactivation of the disease may occur. During prolonged corticosteroid therapy, these patients should receive chemoprophylaxis. Kaposi's sarcoma has been reported to occur in patients receiving corticosteroid therapy. Discontinuation of corticosteroids may result in clinical remission.
Blood and Lymphatic System: Aspirin and nonsteroidal anti-inflammatory agents should be used cautiously in conjunction with corticosteroids.
Immune System Effects: Allergic reactions may occur. Rarely skin reactions and anaphylactic/anaphylactoid reactions have been reported following parenteral methylprednisolone therapy. Physicians using the drug should be prepared to deal with such a possibility. Appropriate precautionary measures should be taken prior to administration, especially when the patient has a history of drug allergy.
Endocrine Effects: Pharmacologic doses of corticosteroids administered for prolonged periods may result in hypothalamic-pituitary adrenal (HPA) suppression (secondary adrenocortical insufficiency). The degree and duration of adrenocortical insufficiency produced is variable among patients and depends on the dose, frequency, time of administration, and duration of glucocorticoid therapy. This effect may be minimized by use of alternate-day therapy.
In addition, acute adrenal insufficiency leading to a fatal outcome may occur if glucocorticoids are withdrawn abruptly. In patients who have received more than physiological doses of systemic corticosteroids (approximately 6mg methylprednisolone) for greater than 3 weeks, withdrawal should not be abrupt. Drug-induced secondary adrenocortical insufficiency may therefore be minimized by gradual reduction of dosage. How dose reduction should be carried out depends largely on whether the disease is likely to relapse as the dose of systemic corticosteroids is reduced.
Clinical assessment of disease activity may be needed during withdrawal. If the disease is unlikely to relapse on withdrawal of systemic corticosteroids, but there is uncertainty about HPA suppression, the dose of systemic corticosteroid may be reduced rapidly to physiological doses.
Once a daily dose of 6mg methylprednisolone is reached, dose reduction should be slower to allow the HPA-axis to recover. Abrupt withdrawal of systemic corticosteroid treatment, which has continued up to 3 weeks is appropriate if it considered that the disease is unlikely to relapse. Abrupt withdrawal of doses up to 32mg daily of methylprednisolone for 3 weeks is unlikely to lead to clinically relevant HPA-axis suppression, in the majority of patients. In the following patient groups, gradual withdrawal of systemic corticosteroid therapy should be considered even after courses lasting 3 weeks or less: Patients who have had repeated courses of systemic corticosteroids, particularly if taken for greater than 3 weeks; When a short course has been prescribed within one year of cessation of long-term therapy (months or years); Patients who may have reasons for adrenocortical insufficiency other than exogenous corticosteroid therapy; Patients receiving doses of systemic corticosteroid greater than 32 mg daily of methylprednisolone; Patients repeatedly taking doses in the evening.
Patients should carry 'Steroid Treatment' cards which give clear guidance on the precautions to be taken to minimise risk and which provide details of prescriber, drug, dosage and the duration of treatment. This type of relative insufficiency may persist for months after discontinuation of therapy; therefore, in any situation of stress occurring during that period, hormone therapy should be reinstituted. Since mineralocorticoid secretion may be impaired, salt and/or a mineralocorticoid should be administered concurrently. In patients on corticosteroid therapy subjected to unusual stress, increased dosage of rapidly acting corticosteroids before, during and after the stressful situation is indicated. A steroid "withdrawal syndrome", seemingly unrelated to adrenocortical insufficiency, may also occur following abrupt discontinuance of glucocorticoids. This syndrome includes symptoms such as: anorexia, nausea, vomiting, lethargy, headache, fever, joint pain, desquamation, myalgia, weight loss, and/or hypotension. These effects are thought to be due to the sudden change in glucocorticoid concentration rather than to low corticosteroid levels. Because glucocorticoids can produce or aggravate Cushing's syndrome, glucocorticoids should be avoided in patients with Cushing's disease. There is an enhanced effect of corticosteroids on patients with hypothyroidism. Frequent patient monitoring is necessary in patients with hypothyroidism.
Metabolism and Nutrition: Frequent patient monitoring is necessary in patients with diabetes mellitus (or a family history of diabetes). Corticosteroids, including methylprednisolone, can increase blood glucose, worsen pre-existing diabetes, and predispose those on long-term corticosteroid therapy to diabetes mellitus.
Psychiatric Effects: Patients and/or carers should be warned that potentially severe psychiatric adverse reactions may occur with systemic steroids. Symptoms typically emerge within a few days or weeks of starting treatment. Risks may be higher with high doses/systemic exposure, although dose levels do not allow prediction of the onset, type, severity or duration of reactions. Most reactions recover after either dose reduction or withdrawal, although specific treatment may be necessary. Patients/carers should be encouraged to seek medical advice if worrying psychological symptoms develop, especially if depressed mood or suicidal ideation is suspected. Patients/carers should be alert to possible psychiatric disturbances that may occur either during or immediately after dose tapering/withdrawal of systemic steroids, although such reactions have been reported infrequently.
Particular care is required when considering the use of systemic corticosteroids in patients with existing or previous history of severe affective disorders in themselves or in their first degree relatives. These would include depressive or manic-depressive illness and previous steroid psychosis. Frequent patient monitoring is necessary in patients with existing or previous history of severe affective disorders (especially previous steroid psychosis).
Nervous System Effects: Corticosteroids should be used with caution in patients with seizure disorders. Frequent patient monitoring is necessary in patients with epilepsy.
Corticosteroids should be used with caution in patients with myasthenia gravis. Frequent patient monitoring is necessary in patients with myasthenia gravis.
Ocular Effects: Frequent patient monitoring is necessary in patients with glaucoma (or a family history of glaucoma) and in patients with ocular herpes simplex, for fear of corneal perforation. Prolonged use of corticosteroids may produce posterior subcapsular cataracts and nuclear cataracts (particularly in children), exophthalmos, or increased intraocular pressure, which may result in glaucoma with possible damage to the optic nerves. Establishment of secondary fungal and viral infections of the eye may also be enhanced in patients receiving glucocorticoids.
Cardiac Effects: Adverse effects of glucocorticoids on the cardiovascular system, such as dyslipidemia and hypertension, may predispose treated patients with existing cardiovascular risk factors to additional cardiovascular effects, if high doses and prolonged courses are used. Accordingly, corticosteroids should be employed judiciously in such patients and attention should be paid to risk modification and additional cardiac monitoring if needed. Low dose and alternate day therapy may reduce the incidence of complications in corticosteroid therapy. There have been a few reports of cardiac arrhythmias and/or circulatory collapse and/or cardiac arrest associated with the rapid intravenous administration of large doses of methylprednisolone (greater than 500mg administered over a period of less than 10 minutes). Bradycardia has been reported during or after the administration of large doses of methylprednisolone sodium succinate, and may be unrelated to the speed and duration of infusion. Systemic corticosteroids should be used with caution, and only if strictly necessary, in cases of congestive heart failure. Care should be taken for patients receiving cardioactive drugs such as digoxin because of steroid induced electrolyte disturbance/potassium loss. Frequent patient monitoring is necessary in patients with congestive heart failure or recent myocardial infarction (myocardial rupture has been reported).
Vascular Effects: Steroids should be used with caution in patients with hypertension. Frequent patient monitoring is necessary.
Gastrointestinal Effects: There is no universal agreement on whether corticosteroids per se are responsible for peptic ulcers encountered during therapy; however, glucocorticoid therapy may mask the symptoms of peptic ulcer so that perforation or haemorrhage may occur without significant pain. Particular care is required when considering the use of systemic corticosteroids in patients with the following conditions and frequent patient monitoring is necessary: Ulcerative colitis; Perforation, Abscess or other pyogenic infections; Diverticulitis; Fresh intestinal anastomoses; Peptic ulceration.
Hepatobiliary Effects: High doses of corticosteroids may produce acute pancreatitis.
Musculoskeletal Effects: Particular care is required when considering the use of systemic corticosteroids in patients with myasthenia gravis or osteoporosis (post-menopausal females are particularly at risk) and frequent patient monitoring is necessary. Osteoporosis is a common but infrequently recognized adverse effect associated with a long-term use of large doses of glucocorticoid.
Renal and Urinary Disorders: Particular care is required when considering the use of systemic corticosteroids in patients with renal insufficiency and frequent patient monitoring is necessary.
Investigations: Average and large doses of hydrocortisone or cortisone can cause elevation of blood pressure, salt and water retention, and increased excretion of potassium. These effects are less likely to occur with the synthetic derivatives except when used in large doses. Dietary salt restriction and potassium supplementation may be necessary. All corticosteroids increase calcium excretion.
Injury, Poisoning and Procedural Complications: Corticosteroids should not be used for the management of head injury or stroke because it is unlikely to be of benefit and may even be harmful.
Other Adverse Events: Since complications of treatment with glucocorticoids are dependent on the size of the dose and the duration of treatment, a risk/benefit decision must be made in each individual case as to dose and duration of treatment as to whether daily or intermittent therapy should be used. The lowest possible dose of corticosteroid should be used to control the condition under treatment and when reduction in dosage is possible, the reduction should be gradual.
Effects on ability to drive and use machine: The effect of corticosteroids on the ability to drive or use machinery has not been systematically evaluated. Undesirable effects, such as dizziness, vertigo, visual disturbances, and fatigue are possible after treatment with corticosteroids. If affected, patients should not drive or operate machinery.
Use in Children: Growth and development of infants and children on prolonged corticosteroid therapy should be carefully observed. Growth may be suppressed in children receiving long-term, daily, divided-dose glucocorticoid therapy and use of such regimen should be restricted to the most urgent indications. Alternate-day glucocorticoid therapy usually avoids or minimizes this side effect. Infants and children on prolonged corticosteroid therapy are at special risk from raised intracranial pressure. High doses of corticosteroids may produce pancreatitis in children.
Use in the Elderly: The common adverse effects of systemic corticosteroids may be associated with more serious consequences in old age, especially osteoporosis, hypertension, hypokalaemia, diabetes, susceptibility to infection and thinning of the skin. Caution is recommended with prolonged corticosteroid treatment in the elderly due to a potential increase risk for osteoporosis, as well as increased risk for fluid retention with possible resultant hypertension. Close clinical supervision is required to avoid life-threatening reactions.
Fertility: There is no evidence that corticosteroids impair fertility. In women treatment with corticosteroids can lead to menstrual irregularities.
Lactation: Corticosteroids are excreted in small amounts in breast milk, however, doses of up to 40mg daily of methylprednisolone are unlikely to cause systemic effects in the infant. Infants of mothers taking higher doses than this may have a degree of adrenal suppression, but the benefits of breast-feeding are likely to outweigh any theoretical risk.
Pregnancy: The ability of corticosteroids to cross the placenta varies between individual drugs, however, methylprednisolone does cross the placenta. Administration of corticosteroids to pregnant animals can cause abnormalities of foetal development including cleft palate, intra-uterine growth retardation and affects on brain growth and development. There is no evidence that corticosteroids result in an increased incidence of congenital abnormalities, such as cleft palate in man, however, when administered for long periods or repeatedly during pregnancy, corticosteroids may increase the risk of intrauterine growth retardation. Hypoadrenalism may, in theory, occur in the neonate following prenatal exposure to corticosteroids but usually resolves spontaneously following birth and is rarely clinically important. As with all drugs, corticosteroids should only be prescribed when the benefits to the mother and child outweigh the risks. When corticosteroids are essential, however, patients with normal pregnancies may be treated as though they were in the non-gravid state. Cataracts have been observed in infants born to mothers undergoing long-term treatment with corticosteroids during pregnancy.
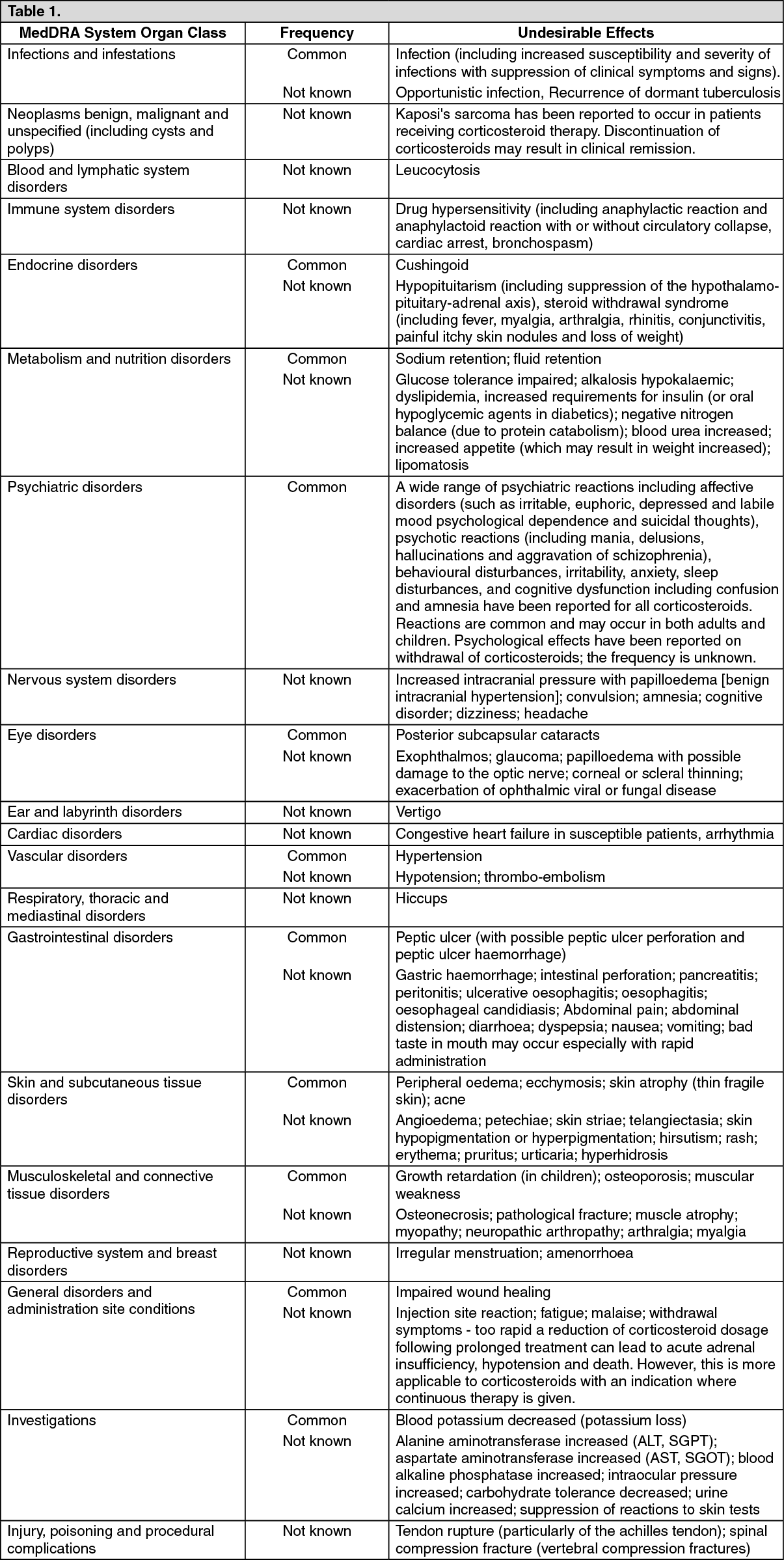
Under normal circumstances methylprednisolone therapy would be considered as short-term. However, the possibility of side-effects attributable to corticosteroid therapy should be recognised, particularly when high-dose therapy is being used. Such side-effects include: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Methylprednisolone is a cytochrome P450 enzyme (CYP) substrate and is mainly metabolized by the CYP3A4 enzyme. CYP3A4 is the dominant enzyme of the most abundant CYP subfamily in the liver of adult humans. It catalyzes 6β-hydroxylation of steroids, the essential Phase I metabolic step for both endogenous and synthetic corticosteroids. Many other compounds are also substrates of CYP3A4, some of which (as well as other drugs) have been shown to alter glucocorticoid metabolism by induction (upregulation) or inhibition of the CYP3A4 enzyme.
CYP3A4 INHIBITORS - Drugs that inhibit CYP3A4 activity generally decrease hepatic clearance and increase the plasma concentration of CYP3A4 substrate medications, such as methylprednisolone. In the presence of a CYP3A4 inhibitor, the dose of methylprednisolone may need to be titrated to avoid steroid toxicity.
CYP3A4 INDUCERS - Drugs that induce CYP3A4 activity generally increase hepatic clearance, resulting in decreased plasma concentration of medications that are substrates for CYP3A4. Co-administration may require an increase in methylprednisolone dosage to achieve the desired result.
CYP3A4 SUBSTRATES - In the presence of another CYP3A4 substrate, the hepatic clearance of methylprednisolone may be inhibited or induced, with corresponding dosage adjustments required. It is possible that adverse events associated with the use of either drug alone may be more likely to occur with co-administration.
NON-CYP3A4-MEDIATED EFFECTS - Other interactions and effects that occur with methylprednisolone are described in table as follows: (See Table 2.)
Click on icon to see table/diagram/image
Corticosteroids antagonize the hypotensive effect of all antihypertensives. There is an increased risk of hypokalaemia when corticosteroids are given with cardiac glycosides. The effects of corticosteroids may be reduced for 3-4 days after mifepristone.
Incompatibilities: To avoid compatibility and stability problems, it is recommended that methylprednisolone sodium succinate be administered separately from other compounds that are administered via the IV route of administration. Drugs that are physically incompatible in solution with methylprednisolone sodium succinate include, but are not limited to: allopurinol sodium, doxapram hydrochloride, tigecycline, diltiazem hydrochloride, calcium gluconate, vecuronium bromide, rocuronium bromide, cisatracurium besylate, glycopyrrolate, propofol.
Store below 30°C.
Solutions reconstituted with the recommended diluents can be stored below 25°C for 48 hours. Freshly reconstituted solution is recommended.
H02AB04 - methylprednisolone ; Belongs to the class of glucocorticoids. Used in systemic corticosteroid preparations.
Vaxcel Methylprednisolone powd for inj 1 g
10 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image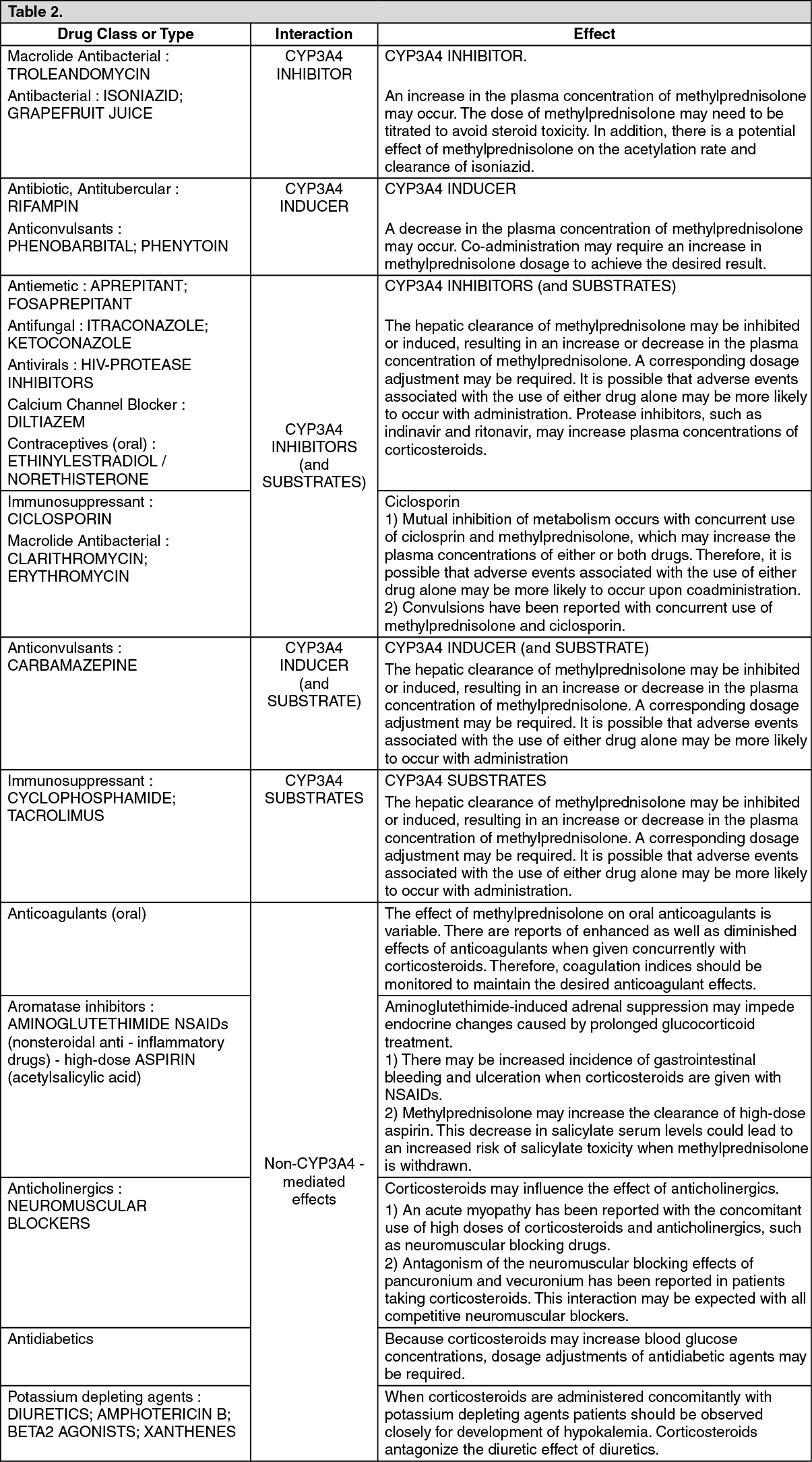 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
